
NETest 2.0®
What is a Neuroendocrine Tumor (NET)?
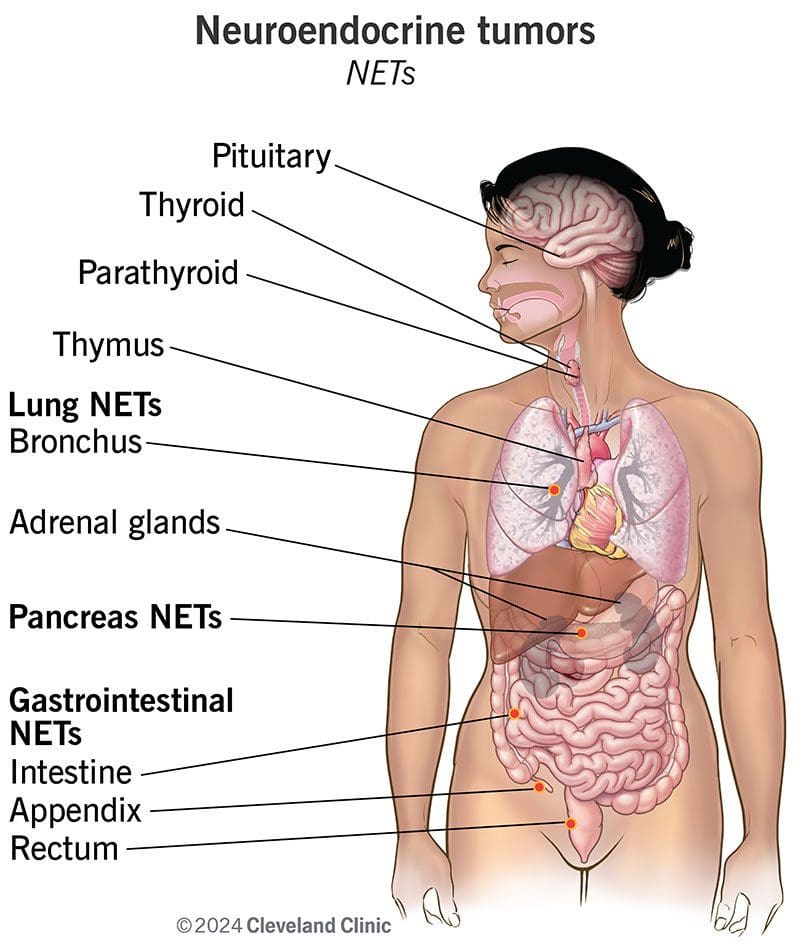
Neuroendocrine tumors (NETs) originate from neuroendocrine cells, which possess both nerve and hormone-producing properties. Found throughout the body, these cells release hormones in response to signals, playing a key role in various physiological processes. NETs can develop in the gastrointestinal tract, pancreas, lungs, and other tissues, ranging from slow-growing to aggressive forms. Although they typically grow slowly, poorly differentiated NETs can be highly aggressive and are known to metastasize, often affecting the liver.
Incidence and Prevalence
The incidence of NETs in the USA has increased significantly, from 1.09 per 100,000 in 1973 to 6.98 per 100,000 in 2012, likely due to improved diagnostics and heightened awareness. Approximately 1 in 3,000 individuals in the USA are living with a NET. Common types include gastrointestinal NETs, particularly in the small intestine, with an incidence of about 3-4 cases per 100,000 annually.
Risk Factors
NETs can occur at any age, peaking between 50 and 65 years. Some studies suggest a slight predominance in women for gastrointestinal NETs, while pancreatic NETs may be more common in men. Racial disparities exist, with higher rates observed in certain groups, such as African Americans for specific NET types.
Risk factors include:
- Genetic: Family history (e.g., MEN1, VHL Disease).
- Environmental: Smoking, chronic gastritis, and long-term use of medications like proton pump inhibitors (PPIs).
- Lifestyle: Hormonal imbalances and chronic inflammatory conditions can increase risk.
Most NETs arise sporadically without clear causes.
Diagnosis and Unmet Needs
Diagnosing NETs typically involves imaging (CT, MRI, PET), biopsy, and biomarker measurements (e.g., chromogranin A). Approximately 50–70% are metastatic at diagnosis, highlighting the need for effective therapies. Current diagnostic tools, including circulating biomarkers, often lack reliability and correlate poorly with treatment responses.
Patient Management
Once diagnosed, NET treatment options include:
- Surgery: Preferred for localized tumors.
- Medications: Somatostatin analogs (e.g., octreotide), targeted therapies (e.g., everolimus), and chemotherapy for aggressive cases.
- Peptide Receptor Radionuclide Therapy (PRRT): Targets tumors using radiolabeled somatostatin analogs.
- Hormonal Control: Essential for managing symptoms in functional NETs.
Prognosis varies based on tumor type and stage, with well-differentiated NETs generally having better outcomes. There remains a critical need for validated non-invasive biomarkers for improved diagnosis, prognosis, and treatment monitoring.
What’s NETest 2.0®?
NETest 2.0® is a test using a simple blood draw. From this blood draw, Wren Laboratories looks for 51 cancer-associated genes related to Neuroendocrine cancer tumors. This is based on very sensitive RNA technologies and can help your doctor determine how to treat your specific tumor, this customized treatment plan, based specifically on your tumor and its behavior, is known as precision medicine.
Here is how it works:
- Your doctor will have a sample of your blood taken. We only require a very small amount for our test.
- Next, your doctor sends your sample and the test order to our laboratory
- We extract the RNA from this small amount of blood sample and run our tests
- We then provide your doctor with information about the status of your cancer. This gives your doctor information to determine what your treatment plan should be
- Your doctor meets with you to discuss the findings and next steps in your care
Why Choose WREN’s NETest 2.0®?
WREN’s NETest 2.0® has been analytically validated and demonstrated its clinical value in over 50 third-party studies, including research from top medical institutions.
The test boasts an analytical accuracy of 94% and precision of 96.7-97.9%, with a high sensitivity capable of detecting 1 cell/mL-RNA equivalent.

Diagnostic Biomarker
94% of patients with a high NETest 2.0® Diagnostic Score are likely to have a NET, while 90% of those with a low score do not.

Prognostic Insights
Patients with high scores face an 80% chance of tumor progression, whereas those with low scores have a 90% chance of stable disease.

Patient Monitoring
Increased Diagnostic Scores in serial samples detect minimal residual disease (MRD) or tumor recurrence in 84% of cases.
Predictor of Treatment Response
NET patients with a positive Peptide Receptor Radionuclide Therapy (PRRT) Predictive Quotient (PPQ) score have a 95% likelihood of benefiting from targeted therapeutics (e.g., Lutathera®), compared to just 10% in PPQ-negative patients.
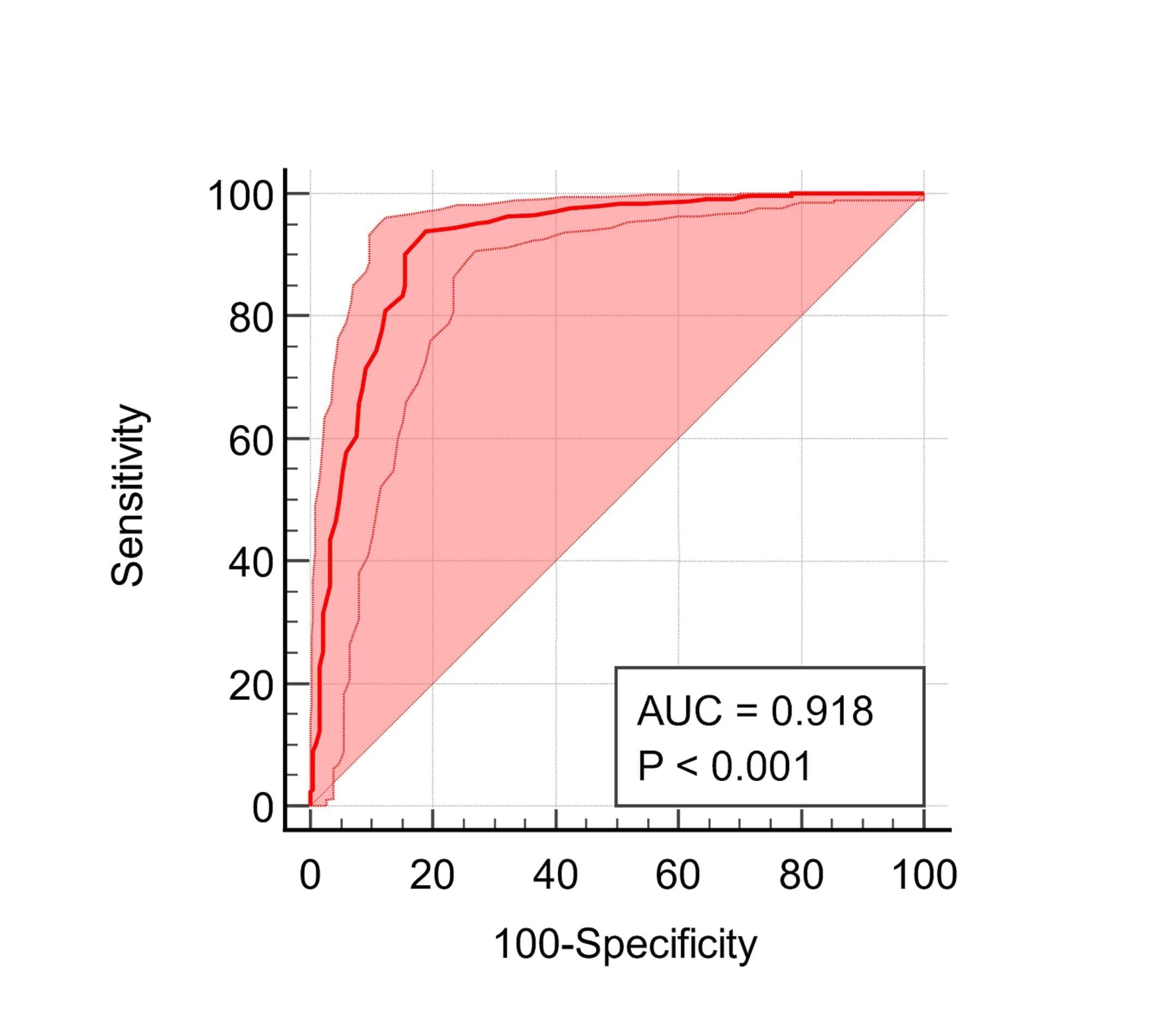
Diagnostic Score
A high PROSTest score indicates a 93% likelihood of prostate cancer, while a low score suggests a 90% chance of not having the disease.
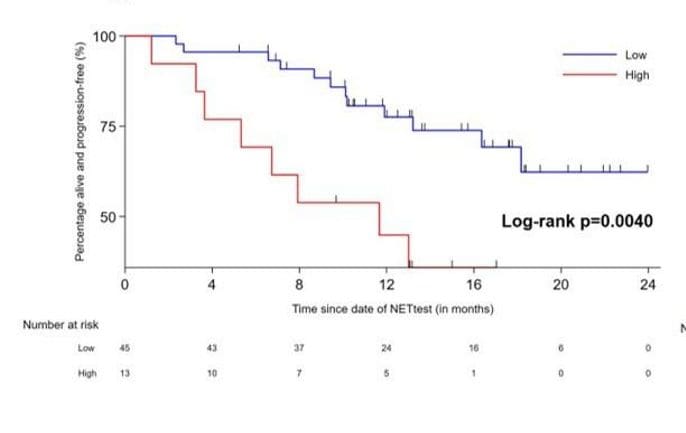
Prognostic Score
Based on a subset of genes, also ranging from 0-100, with a cutoff of 40 to distinguish between progressive and stable disease.
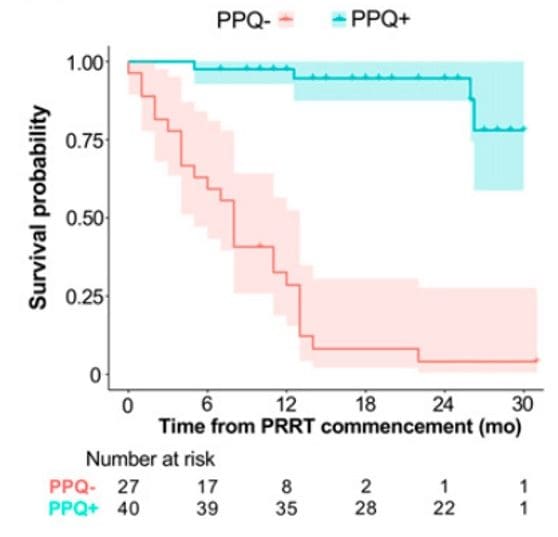
PPQ Score
Peptide Receptor Radionuclide Therapy (PRRT)-Predictive Quotient, ranging from 0-100, with a cutoff of 50 to predict the likelihood of response to PRRT (PPQ+ vs. PPQ-).
